From Dr. Erin:
The last few days have been even busier than usual at the sanctuary!
Both Jamie and Foxie had complete exams this week. The decision to anesthetize any of the chimps is never taken lightly but when it comes to anesthetizing older chimps (Jamie is turning 48 in a couple weeks and Foxie is 49), we are especially careful and consider several factors before making the decision to perform an exam under anesthesia. These factors include what data we can get through positive reinforcement training, how long it’s been since their last exam, as well as any previous health concerns or current changes in behavior or affect that indicates there may be a health concern.
In Jamie’s case, as J.B. noted in a previous blog post, Jamie has been slowing down over the last several months and her belly has become more pronounced. While the physical changes can certainly be ascribed to aging (ask me how I know) and the change in social structure since Jody’s passing, we couldn’t be sure and there was something “off” enough about her that an exam was warranted.
With Foxie, we were concerned about a cough that developed this past summer and persisted in spite of various medications to address possible causes.
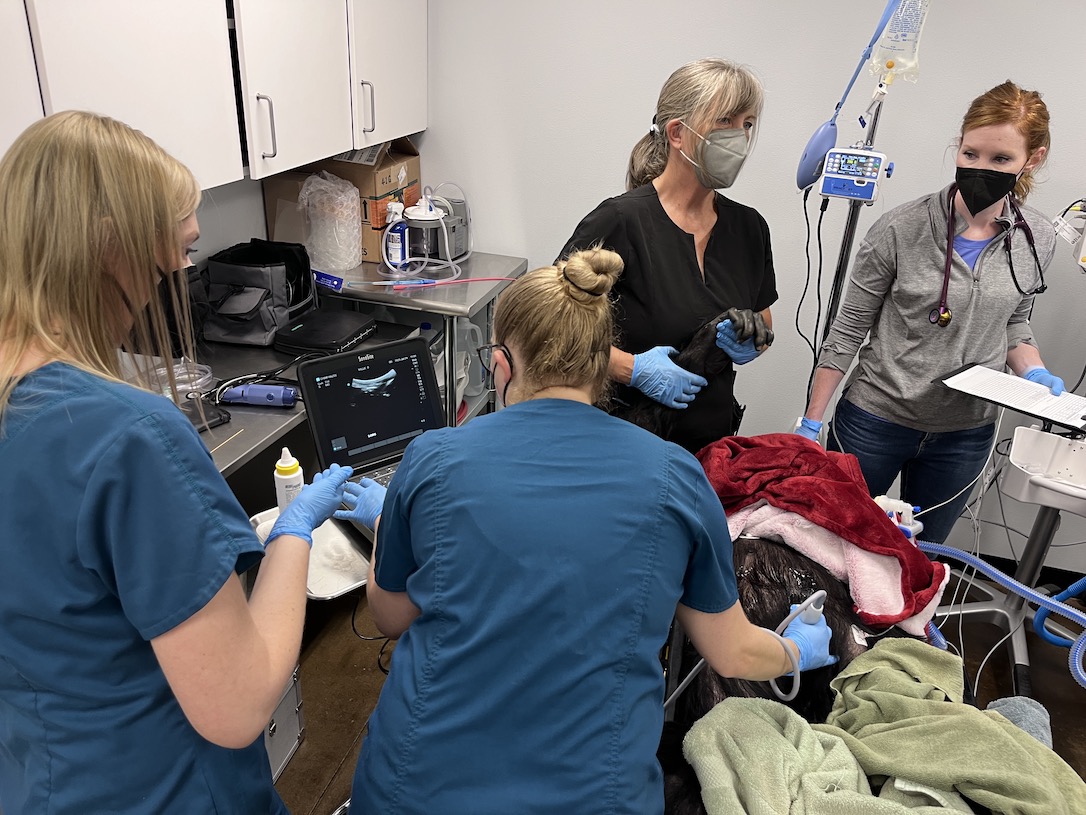
Both chimps did well under anesthesia and while Jamie wanted an extra day of rest before rejoining the group, Foxie was clamoring to be back with her family before breakfast this morning. The procedures consisted of a complete dental exam, including x rays and cleaning, abdominal ultrasound, echocardiogram, head to toe physical, full body x rays, and sample collection for diagnostic tests on blood, respiratory fluid and urine.
Jamie’s team on Friday included local professionals Dan Whitemarsh, DDS and Tanya Hebert, sonographer. Traveling from west of the Cascades were Jaime Sheehan, echo tech, Milo Torres, LVT & the wonderful Dr. Dan Low and anesthesiology intern Pat Herndon. Dr. Yousuf Jafarey, an experienced primate vet and dear friend, flew up from California just to participate in the exams!
Jaime Sheehan returned yesterday to perform Foxie’s echo as well. The rest of Foxie’s team consisted of Dr. Charles Dyer, the dentist from the Dental Coalition for Conservation (who performed in Missy’s dental care in July), Korey Krause, sonographer from Kittitas Valley Health, David Liston, MD and Kate Uselman, CRNA from Seattle on anesthesia, as well as Dr. Jafarey and myself.
We have some preliminary information from the exams that will help guide care for both of these amazing older ladies and are awaiting lab results, radiology, and cardiology reviews that will further inform protocols for keeping them as comfortable as possible in their golden years.
I am incredibly grateful to the professionals that lend their time, effort and expertise to these exams, it really is a team effort to ensure the chimps have the safest and most thorough exam possible. I am so appreciative and impressed by the staff and volunteers who rearrange schedules, take on extra work, come in early, deal with clinic equipment spilling into the foyer and all support each other as well as the chimps. I work with the most wonderful people!
And we are so fortunate to work with the incomparable Dr. Erin!
The team prepares blood samples:

Jamie’s teeth are examined and cleaned while she is given an abdominal ultrasound:



The team monitors Jamie during recovery:

Jamie sleeps off the events of the day:

Foxie receives a dental cleaning and abdominal ultrasound:

X-rays are taken of Foxie’s teeth:

Nothing speeds up recovery like some pudding in a cup:

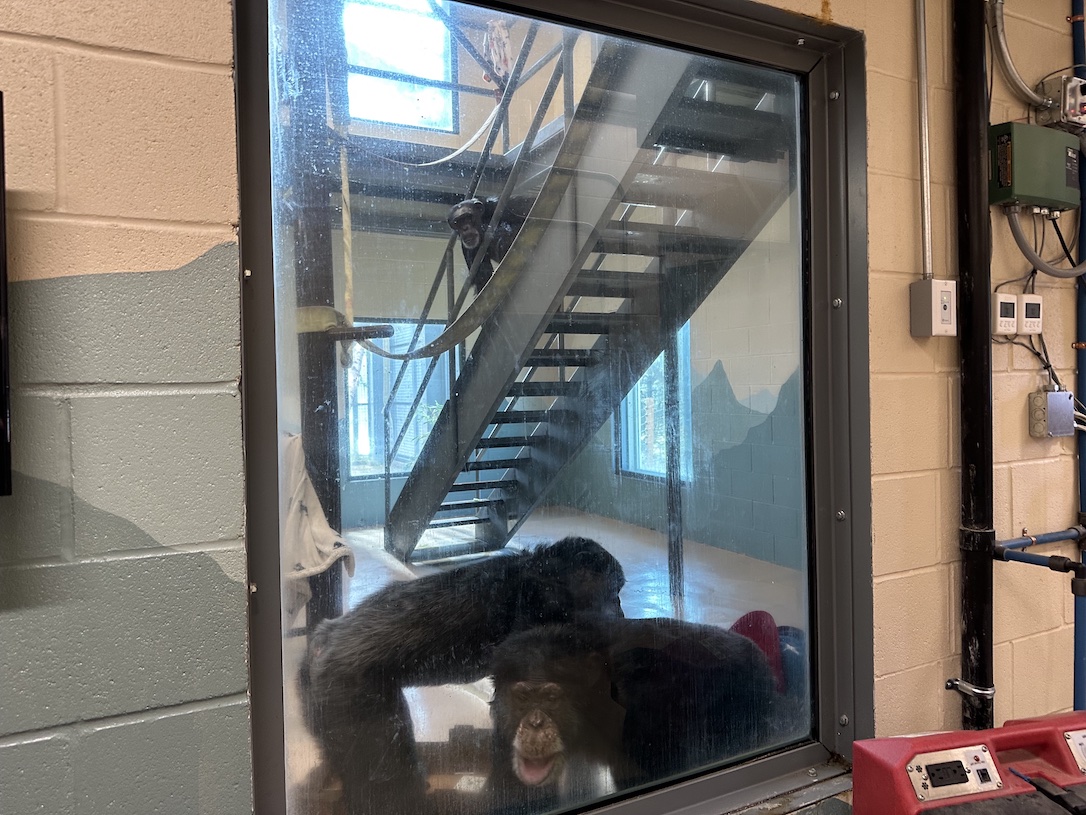
Jamie and Foxie enjoying a lunch forage on the hill this afternoon: